The temporomandibular joint — universally referred to by its initials TMJ — is one of the most complex and heavily used joints in the human body. Connecting the lower jaw (mandible) to the skull on both sides of the face, it operates continuously throughout every waking hour: during speech, chewing, swallowing, and even during sleep in people who grind or clench their teeth. When this intricate joint system and the muscles that drive it malfunction, the result is a constellation of symptoms grouped under the term temporomandibular disorder (TMD) that frequently includes significant headache pain.
The relationship between temporomandibular disorders and headache is both direct and indirect, and the two conditions influence each other in ways that have only been fully appreciated through research conducted in the past two decades. Head pain is one of the three most common symptoms reported by TMD patients alongside jaw pain and restricted jaw movement, and the headaches associated with TMD have characteristics that distinguish them from primary headache disorders, though they can coexist with and complicate the management of migraine and tension-type headache and buy fioricet online in the same individual.
The anatomical basis for TMD-associated headache lies primarily in the shared innervation of the jaw structures and the head by the trigeminal nerve. The temporalis muscle — a large fan-shaped muscle that originates from the temporal bone of the skull and inserts on the mandible — is the primary muscle of jaw closure and is frequently affected in TMD. When this muscle develops trigger points, sustained contractions, or inflammatory changes due to jaw dysfunction, the pain is referred into the temporal region of the head in a distribution that precisely mimics tension-type headache. Similarly, the masseter muscle, which runs along the outer jaw and performs the bulk of the chewing force, refers pain upward into the cheek, lower molars, and, when severely affected, into the temporal and parietal regions of the skull.
Population studies indicate that approximately 5 to 12 percent of the general population has some form of temporomandibular disorder significant enough to produce symptoms, with TMD-associated headache present in a substantial proportion of those affected. Women are diagnosed with TMD roughly twice as frequently as men, a disparity that researchers have linked to hormonal influences on tissue laxity, pain sensitivity, and the social factors that influence care-seeking behavior.
Clinical Features of TMD-Associated Headache
TMD-associated headache has several clinical features that help identify it, though these features must be interpreted alongside the broader clinical picture to arrive at an accurate diagnosis. The headache is typically located in the temporal region — the area of the skull above and in front of the ear — and may extend into the cheek, preauricular area, and lower face on the same side. In patients with bilateral TMD, the headache may affect both temporal regions, though often asymmetrically.
The quality of the pain is typically dull, aching, and pressure-like rather than pulsating. Critically, the headache is associated with jaw use: chewing tough foods, prolonged talking, singing, or any activity that extensively engages the jaw muscles tends to provoke or worsen the pain. Many patients note that their headache is consistently worse in the morning, particularly if they grind or clench their teeth during sleep — a condition called bruxism — which produces sustained isometric jaw muscle contraction throughout the night and results in muscle fatigue and pain upon awakening.
The International Classification of Headache Disorders includes headache attributed to temporomandibular disorder as a secondary headache diagnosis, requiring that the headache developed in temporal relation to the onset of the TMD, that the headache is reproduced or exacerbated by jaw movement, and that the temporal relationship and improvement with TMD treatment confirm the diagnosis.
Physical examination findings in TMD include tenderness on palpation of the masticatory muscles, reduced or painful jaw opening, deviation of the jaw on opening, clicking or popping sounds from the TMJ during movement (joint sounds), and in some cases, a palpable disc displacement within the joint. Occlusal examination may reveal evidence of bruxism including tooth wear facets, and the dentist or oral medicine specialist examining the patient may identify malocclusion or other dental factors contributing to jaw muscle overload.
Why TMD and Primary Headache Disorders Coexist So Frequently
One of the most clinically significant findings in contemporary TMD research is the remarkably high comorbidity rate between TMD and primary headache disorders, particularly migraine. Studies examining the prevalence of migraine in TMD patients consistently find rates two to three times higher than in the general population, and conversely, migraine patients show significantly elevated rates of TMD diagnosis compared to matched non-headache controls.
Several mechanisms likely explain this bidirectional comorbidity. Central sensitization, discussed in the context of other headache types, is relevant here: the prolonged pain input from TMD into the trigeminal system can lower the threshold for migraine attacks by contributing to trigeminal sensitization. Simultaneously, the repeated trigeminal activation of migraine attacks may sensitize the trigeminal processing of jaw-related pain, making TMD pain more severe and longer-lasting in migraine patients than it would be in non-migraineurs.
Shared neurobiological predispositions — including variations in pain regulatory genes, differences in descending pain inhibition efficiency, and autonomic nervous system dysregulation — may create a common vulnerability to both conditions. The genetic studies examining migraine and TMD separately have identified overlapping biological pathways, suggesting that part of the comorbidity reflects shared underlying susceptibility rather than a simple causal relationship in one direction.
Psychological factors including anxiety, depression, and somatization play important roles in both conditions and may be part of the shared vulnerability. Catastrophizing — a cognitive pattern characterized by the tendency to focus on pain and view it as overwhelming — predicts both the development of chronic TMD and the severity and disability associated with migraine, suggesting that psychological factors are not merely consequences of these painful conditions but active contributors to their chronification.
Diagnosis and the Role of Multidisciplinary Assessment
Accurate diagnosis of TMD-associated headache requires collaboration between dentists or oral medicine specialists and headache neurologists. The Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD), recently updated to the DC/TMD, provides a standardized systematic approach to TMD diagnosis that assesses both the physical findings and the psychological factors relevant to prognosis and treatment planning.
Imaging plays a selective role in TMD diagnosis. Panoramic dental radiographs provide an overview of jaw structures but have limited sensitivity for intraarticular pathology. Cone-beam computed tomography offers better osseous detail and can reveal bony changes in the condyle and articular eminence. MRI of the temporomandibular joints is the gold standard for evaluating disc position and morphology, joint effusion, and other intraarticular soft tissue findings. However, imaging findings must always be correlated with clinical symptoms since asymptomatic disc displacement and other radiographic findings are common in the general population.
The differential diagnosis of temporal headache must carefully consider whether the pain arises from the TMJ and masticatory muscles, from cervical structures (cervicogenic headache), from the temporalis muscle alone as part of a tension-type headache without TMD, from primary migraine affecting the temporal distribution, or from combinations of these mechanisms operating simultaneously — as is common in complex patients seen in tertiary headache centers.
Treatment: An Integrated Approach
Effective treatment of TMD-associated headache requires an integrated strategy that simultaneously addresses the jaw dysfunction and the pain it generates. Oral appliance therapy — specifically intraoral splints custom-fitted by a dentist or oral medicine specialist — represents the cornerstone of TMD management. The most commonly used appliance covers the upper or lower teeth, establishes a controlled occlusal position that reduces loading on the TMJ, and limits the mechanical damage of nocturnal bruxism. Evidence from randomized trials supports the efficacy of stabilization splints in reducing both jaw pain and associated temporal headache.
Physical therapy for the jaw and cervical spine is an essential complementary treatment. Manual therapy techniques targeting the masticatory muscles and the cervical and thoracic spine address the muscular contributors to pain, restore normal jaw mechanics, and reduce referred headache pain. Exercises to strengthen and coordinate jaw muscles, improve posture, and reduce parafunctional habits are taught and reinforced across treatment sessions.
Pharmacological management for the headache component is guided by the same phenotypic principles described in the post-traumatic headache section: treatment is selected based on the clinical character of the associated headache. Muscle relaxants can be particularly helpful in the acute period, addressing the jaw muscle spasm and tension that directly contributes to temporal headache. For nocturnal bruxism, low-dose tricyclic antidepressants have both analgesic and muscle-relaxing properties that make them valuable for nighttime use. Botulinum toxin injections into the masseter and temporalis muscles offer an increasingly used and well-evidenced treatment option for refractory TMD-associated headache, reducing the excessive muscle contraction that drives both joint overloading and referred head pain.
Building Long-Term Resilience Against Stress Headache
The ultimate goal of stress-related headache management is building sustainable resilience — a combination of biological, psychological, and behavioral capacities that reduces long-term vulnerability to stress-induced pain. This process requires sustained engagement over months rather than immediate results, and its benefits compound progressively over time rather than being exhausted with use.
Physical resilience — maintaining cardiovascular fitness through regular aerobic exercise, ensuring adequate sleep duration and quality, staying consistently hydrated, and maintaining stable meal timing — creates a physiological foundation that reduces the reactivity of the trigeminal pain system to stress. Research on exercise as a headache preventive is particularly compelling: regular moderate-intensity aerobic exercise performed three to five times per week for 30 or more minutes per session produces headache frequency reductions comparable to some preventive medications in controlled trials, alongside benefits for sleep quality, mood stability, stress tolerance, and cardiovascular health.
Psychological resilience — developed through consistent mindfulness practice, the cognitive restructuring skills of cognitive-behavioral therapy, cultivation of supportive relationships, and engagement in meaningful activities that generate positive emotion independently of pain — reduces the hypervigilance and anxiety sensitivity that amplify the relationship between stress and headache. Patients who develop equanimity toward occasional headache — accepting its presence, using effective treatment without alarm, and returning promptly to valued activities — experience less total suffering and functional disruption than those whose response to headache remains dominated by fear and anticipatory dread.
The integration of these resilience-building practices into daily routine, treated as habitual self-care rather than burdensome medical obligations, creates the conditions for a trajectory of gradual but meaningful improvement in headache frequency and quality of life over the months and years following initial treatment.
Headache in Older Adults: An Often Overlooked Clinical Challenge Headache disorders do not end at retirement age. While the peak prevalence of migraine occurs in […]
Chronic Tension Headache: Definition, Prevalence, and Impact Chronic tension-type headache (CTTH), defined by the International Headache Society as tension headache occurring on 15 or more […]
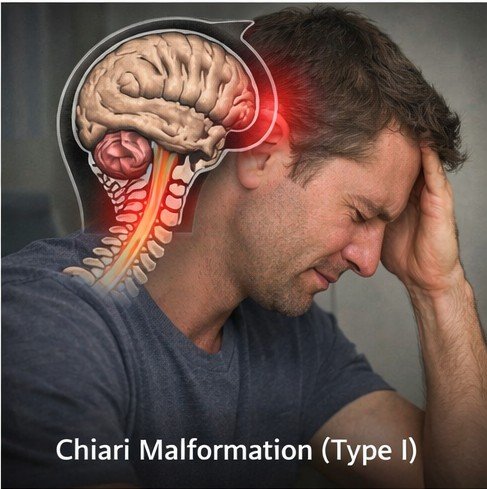
Chiari malformation Type I is a structural neurological condition defined by the downward displacement of the cerebellar tonsils — the lower rounded portions of the […]