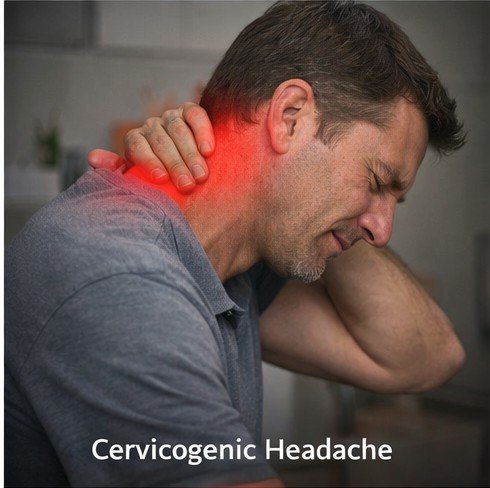
Cervicogenic headache is one of the most consistently misdiagnosed conditions in modern clinical medicine. The term itself describes precisely what is happening physiologically: the pain originates not in the brain, not in the cranial blood vessels, and not in the skull itself — it originates in the cervical spine, the muscles surrounding it, or the complex network of nerves and joints in the neck. Despite this straightforward etymology, many patients spend years receiving treatments directed at their head while the actual structural problem in their neck continues untreated and, in many cases, worsening with time.
The cervical spine consists of seven vertebrae designated C1 through C7. The upper three segments — C1, C2, and C3 — are intimately connected to the trigeminal nerve system via a neurological junction known as the trigeminocervical nucleus. Buy Fioricet online help to this. This anatomical convergence is the biological explanation for why pain arising from neck structures is perceived by the brain as headache pain. When joints, discs, muscles, or nerves in the upper cervical region become irritated, inflamed, or mechanically compromised, the nervous system routes that pain signal through shared pathways that the brain interprets as originating in the head. This is a phenomenon called referred pain, and it is the cornerstone of understanding cervicogenic headache.
Cervicogenic headache accounts for approximately four to eight percent of all headache presentations, though many researchers believe this figure significantly underestimates the true prevalence due to widespread diagnostic confusion with migraine and tension-type headache. The condition affects women roughly four to five times more frequently than men, and the peak incidence occurs between the ages of 30 and 50 — the most productive decades of a person’s professional and personal life.
Identifying the Clinical Features
The clinical presentation of cervicogenic headache has several characteristics that distinguish it from other primary headache disorders, though these distinctions require careful clinical assessment to identify correctly. The pain is almost always unilateral — meaning it affects only one side of the head — and critically, it consistently affects the same side during each episode. This lateralization is a significant diagnostic clue. In migraine, although pain may predominate on one side in a given attack, it can alternate sides across different episodes. In cervicogenic headache, the affected side mirrors the side of the neck pathology and typically remains constant.
The pain typically begins in the upper neck or the region just below the skull — the suboccipital area — and radiates forward toward the forehead, temple, or eye region on the same side. Patients frequently describe a dull, non-throbbing, steady aching quality rather than the pulsating character that typifies migraine. The intensity is usually moderate, though it can become severe during flare-ups or with prolonged physical activity.
One of the most diagnostically useful features is that neck movement consistently triggers, worsens, or reproduces the headache. Turning the head, extending the neck backward, sustaining a flexed neck posture for prolonged periods, or applying manual pressure to specific points in the suboccipital or upper cervical region all typically provoke or intensify the pain. This mechanical reproducibility — the ability to make the headache worse or better by manipulating the neck — is something physicians specifically look for when evaluating a patient for cervicogenic headache.
Restricted range of motion in the cervical spine is another characteristic finding. Patients often note stiffness when turning their head, and a trained clinician performing a passive examination will detect reduced mobility and reproduce pain with specific cervical movements. Some patients also experience associated symptoms including ipsilateral shoulder pain, arm discomfort, blurred vision on the affected side, dizziness, and noise sensitivity — symptoms that frequently lead to a misdiagnosis of migraine in less experienced clinical settings.
Root Causes and Contributing Factors
The structural causes of cervicogenic headache are diverse, reflecting the complexity of the cervical spine as a mechanical system bearing the full weight of the head approximately 24 hours a day. Cervical facet joint dysfunction is among the most common etiological factors. The facet joints — small paired joints at the back of each vertebral level — can develop osteoarthritis, become inflamed after injury, or undergo cartilage degeneration that causes pain with movement. The C2-C3 facet joint is the most frequently implicated level in cervicogenic headache.
Intervertebral disc pathology in the upper cervical spine represents another major cause. Disc degeneration, herniation, or loss of disc height alters the biomechanics of the cervical segment, increasing stress on adjacent joints and nerve roots. Whiplash injuries — sudden, forceful flexion-extension movements of the neck that commonly occur in rear-end motor vehicle collisions — are a leading precipitating event. Post-whiplash cervicogenic headache can develop immediately or, more insidiously, emerge weeks to months after the original trauma as inflammation evolves and structural changes develop.
Postural factors play an increasingly prominent role in contemporary society. The widespread adoption of smartphones, tablets, and desktop computers has created what researchers now call “tech neck” — a posture characterized by forward head position and prolonged cervical flexion. For every inch that the head shifts forward from its neutral position, the effective weight that the cervical spine must support increases by approximately ten pounds. Sustained in this position for hours daily across years, this mechanical stress predisposes individuals to the exact cervical joint and muscle pathology that causes cervicogenic headache.
Muscle factors are important contributors as well. The suboccipital muscle group — a complex of four small paired muscles located at the very base of the skull — is particularly prone to developing trigger points, areas of localized muscle tightness that radiate pain in characteristic patterns when compressed. Trigger points in the suboccipital muscles typically produce pain that wraps around the head from the occiput to the frontal region, a distribution that closely mimics tension headache and can be confused with cervicogenic headache or, when occurring together, represents a combination of both.
Diagnosis: A Process Requiring Clinical Precision
Establishing an accurate diagnosis of cervicogenic headache requires a systematic clinical approach because no single imaging test or blood marker definitively confirms the condition. The International Headache Society has established diagnostic criteria that require: headache caused by a disorder of the cervical spine, evidence of the causative lesion on imaging or clinical examination, abolition of the headache following diagnostic blockade of the suspected cervical structure, and consistent unilaterality without side-shift.
Physical examination by a trained clinician — whether a neurologist, physiatrist, or musculoskeletal specialist — is central to diagnosis. Provocative maneuvers that reproduce the headache by stressing specific cervical segments, palpation of painful and restricted cervical joints, and assessment of neck range of motion provide crucial diagnostic information. The Flexion-Rotation Test is one standardized examination technique particularly useful for identifying C1-C2 dysfunction; restricted and painful range in this test correlates strongly with cervicogenic headache.
Imaging studies including cervical spine radiographs, MRI, and CT scanning can reveal structural abnormalities — disc degeneration, osteophyte formation, facet joint hypertrophy — but findings must be interpreted in the context of clinical symptoms since degenerative changes are extremely common in the general population and frequently asymptomatic. Diagnostic nerve blocks, performed by injecting local anesthetic around specific cervical nerve roots or into facet joints under fluoroscopic or ultrasound guidance, serve as both a diagnostic tool and, when using corticosteroids, a therapeutic intervention.
Treatment Approaches and Management Strategies
The management of cervicogenic headache is most effective when it combines multiple therapeutic approaches targeting both the structural source and the neurological sensitization that develops with chronic pain. Physical therapy is typically the first-line treatment recommendation and forms the cornerstone of long-term management. A structured program targeting the cervical spine and surrounding musculature should include manual therapy techniques — including cervical joint mobilization and manipulation performed by a trained physical therapist — specific strengthening exercises for the deep cervical flexor muscles, and postural re-education to address the mechanical stressors that may have initiated or perpetuated the problem.
Pharmacological management plays an important supporting role. Nonsteroidal anti-inflammatory drugs help reduce local inflammation in cervical joints. Muscle relaxants address the associated cervical muscle tension. When simple analgesics prove insufficient to provide adequate relief during moderate to severe episodes, combination analgesic preparations containing agents that address both the musculotendinous and pain-sensitization components of cervicogenic headache can be an appropriate component of a physician-supervised treatment plan.
Interventional procedures offer more targeted relief for patients with identifiable structural causes. Cervical medial branch nerve blocks, targeting the nerves that supply the facet joints, can provide diagnostic confirmation and sustained pain relief. For patients who respond well to nerve blocks, radiofrequency ablation of the medial branch nerves offers longer-lasting relief by interrupting the pain signal at its source for periods of six months to two years. Greater occipital nerve blocks — injections of local anesthetic and corticosteroid around the greater occipital nerve as it exits the suboccipital region — are frequently used and well-tolerated procedures that can produce substantial headache relief.
Botulinum toxin injections into the cervical muscles represent another intervention with growing evidence in cervicogenic headache. By temporarily reducing the contractile activity of muscles that may be contributing to joint stress and referred pain, botulinum toxin can interrupt the pain cycle and allow the nervous system to desensitize. The injection sites target the suboccipital, trapezius, and sternocleidomastoid muscles based on the individual patient’s pattern of pain.
Long-term management invariably requires attention to lifestyle and ergonomic factors. Workstation assessment and modification to promote a neutral cervical posture, regular movement breaks during prolonged sitting, sleep position optimization using appropriate cervical pillows, and sustained home exercise programs all contribute to preventing recurrence and maintaining the gains achieved through active treatment.
Living Well with Cervicogenic Headache
Cervicogenic headache is a condition that, with accurate diagnosis and appropriate multimodal treatment, can be effectively managed in the vast majority of patients. The key to successful outcomes lies in correct identification of the cervical source, targeted treatment of that structural cause, and rehabilitation of the biomechanical and postural factors that perpetuate the problem. Patients who commit to an active rehabilitation approach — performing their home exercise programs consistently, modifying problematic postures and work habits, and engaging regularly with their treatment team — achieve substantially better long-term outcomes than those who rely exclusively on passive treatments.
It is important for patients with cervicogenic headache to work closely with a healthcare provider experienced in this condition to ensure the diagnosis is confirmed and the treatment plan is individualized to their specific anatomy and lifestyle needs. The overlap with other headache types means that diagnostic precision is essential before committing to a treatment strategy. With the right approach, most patients with cervicogenic headache experience meaningful and lasting reduction in their pain burden.
Patient Education: The Most Powerful Tool for Recovery
Patient education is among the most effective therapeutic interventions for medication overuse headache, yet it remains underutilized in clinical practice. When patients genuinely understand the biological mechanism by which their medication worsens their headache — not because they are weak or morally deficient but because repeated pharmacological manipulation of the brain produces predictable neurochemical adaptations — they develop a fundamentally different relationship with both their pain and their medication choices.
Informed patients recognize the early warning signs of developing overuse before a full chronic daily headache pattern is established. They understand why the two-to-three days per week limit on acute medication exists, and they can apply that understanding to resist the temptation of early dosing during the difficult withdrawal period. They are more likely to persist through the challenging withdrawal process because they have realistic expectations about its duration and the timeline of improvement that follows. Educational interventions delivered at the time of withdrawal initiation, supported by written materials and clinical follow-up, significantly reduce relapse rates compared to withdrawal conducted without education.
Support communities — whether in person or online — provide peer understanding and practical shared experience that clinical encounters alone cannot replicate. Patients who connect with others who have successfully navigated the overuse cycle find both motivation and specific strategies that clinician advice does not always convey. The normalization of the experience — learning that many others have been trapped in the same cycle and found their way out — counters the shame that many medication overuse headache patients carry and that can become a barrier to seeking and sustaining treatment.
The neck bears the weight of the head — averaging approximately five kilograms — through a complex architecture of vertebrae, intervertebral discs, facet joints, ligaments, […]
Tension-type headache is the most prevalent neurological disorder in the world, affecting an estimated seventy-five percent of the general adult population at some point in […]
Stress-induced muscle contraction headache — the clinical syndrome in which sustained psychological stress directly drives the pericranial and cervical muscle hypertonicity that generates or perpetuates […]