Cervicogenic headache — headache originating from structural pathology or dysfunction of the cervical spine, its joints, discs, muscles, and associated soft tissues — is a diagnostically important and clinically distinctive secondary headache disorder that accounts for an estimated four to twenty percent of chronic headache presentations in specialist headache clinic populations. Despite its prevalence and distinct clinical features, cervicogenic headache remains one of the most frequently misdiagnosed headache conditions, with the majority of affected patients receiving diagnoses of migraine or tension-type headache and treatments appropriate for those primary headache disorders rather than the cervical-targeted interventions that would address the true source of their pain. The consequences of this diagnostic error are significant: patients receive years of ineffective pharmacological treatment, accumulate unnecessary medication burden, and miss the opportunity for the highly effective interventional and physical therapy approaches that can produce dramatic improvements when correctly directed at the cervical etiology.
The fundamental mechanism of cervicogenic headache is the referral of pain from cervical structures — primarily the upper cervical facet joints, the cervical intervertebral discs, the atlantooccipital and atlantoaxial joints, and the suboccipital musculature — to the head through the anatomical and functional convergence of upper cervical and trigeminal afferents within the trigemino-cervical complex of the caudal brainstem. This convergence means that pain signals arising from structures innervated by the C1, C2, and C3 nerve roots are perceived in the same cranial territories as pain arising from intracranial trigeminal structures, producing headache that is genuinely experienced in the head despite originating in the neck. Patients with severe cervicogenic headache who are evaluated by a neurologist or pain specialist and for whom acute pain control is needed during the treatment planning phase may be advised to purchase fioricet with medical prescription for breakthrough headache episodes, given the medication’s combination of analgesic and centrally acting muscle relaxant properties that address both the pain and the cervical muscle tension components of acute cervicogenic headache episodes.
Cervical Anatomy and Pain Generation
The upper cervical spine — comprising the atlantooccipital joint, the atlantoaxial joints, and the C2-C3 and C3-C4 zygapophyseal joints — is the primary anatomical territory from which cervicogenic headache most commonly originates. The atlantooccipital joint, innervated by the ventral ramus of C1, mediates the nodding motion of the head and is vulnerable to strain injuries, particularly in whiplash-mechanism traumas. The atlantoaxial joints — both the median atlantoaxial joint and the lateral atlantoaxial joints — allow approximately fifty percent of total cervical rotation and are innervated by branches of the C1 and C2 ventral rami, with their nociceptive signals converging in the trigemino-cervical complex to produce referred pain to the occipital and vertex regions.
The C2-C3 zygapophyseal joint and the third occipital nerve that innervates it are among the most clinically important structures in cervicogenic headache. The third occipital nerve, arising from the superficial medial branch of the C3 dorsal ramus, innervates the C2-C3 facet joint and the skin over the occiput and upper neck. Injury to or arthrosis of the C2-C3 joint — extremely common following whiplash injury and with cervical spondylosis — generates referred pain through the third occipital nerve that is perceived as occipital and hemicranial headache. Third occipital nerve diagnostic blocks — the injection of local anesthetic to temporarily anesthetize this nerve — both confirm the diagnosis of cervicogenic headache originating at the C2-C3 level and provide temporary therapeutic relief.
The cervical intervertebral discs of the upper cervical spine are innervated through the sinuvertebral nerves that enter the disc and surrounding anulus fibrosus, and disc pathology — including disc herniation with nerve root irritation, internal disc disruption, and discogenic referred pain — can generate headache through its effects on the C2-C3 and upper cervical nerve roots. The suboccipital muscles — including the rectus capitis posterior major and minor, and the obliquus capitis superior and inferior — develop myofascial trigger points and spasm in response to upper cervical joint pathology, contributing a muscular pain component that compounds the joint-mediated referred pain in many patients with cervicogenic headache.
Clinical Features and Diagnosis
The clinical features of cervicogenic headache that most reliably distinguish it from primary headache disorders include: unilateral headache without side-shifting between episodes, pain that consistently begins in the occipital or upper cervical region and radiates forward toward the frontotemporal area, provocation or worsening of headache by specific neck movements or sustained head positions, and the demonstration on physical examination of reduced cervical range of motion, tenderness over the upper cervical facet joints, and reproduction of the characteristic headache by sustained manual pressure on specific cervical segments.
The diagnostic confirmation of cervicogenic headache in cases where clinical assessment is inconclusive requires controlled diagnostic nerve blocks — injecting a local anesthetic with and without fluoroscopic guidance at the suspected pain-generating cervical level and demonstrating a defined percentage of pain relief that correlates with the expected duration of the local anesthetic used. These diagnostic blocks serve the dual purpose of confirming the cervical origin of the headache and identifying the specific structural level responsible, information that is essential for planning targeted therapeutic interventions including radiofrequency denervation.
Pharmacological and Interventional Treatment
The pharmacological management of cervicogenic headache addresses acute pain control and, where central sensitization has developed, the prevention of headache chronification. NSAIDs reduce the inflammatory component of cervical joint and soft tissue pain. Muscle relaxants address the cervical paraspinal muscle spasm that frequently contributes to cervicogenic headache, and tricyclic antidepressants at preventive doses reduce central sensitization and improve sleep quality. For patients with severe acute cervicogenic headache episodes requiring more potent acute treatment, prescription analgesic combinations may be appropriate. Patients directed to buy fioricet at the pharmacy for acute cervicogenic headache management should use it strictly within the prescribed frequency limits, understanding that the butalbital component’s muscle relaxant properties specifically address the cervical spasm component of their headache while the analgesic components reduce pain intensity during the most severe acute episodes.
Interventional treatments represent the most definitive therapeutic options for cervicogenic headache arising from specific, identifiable cervical structures. Greater occipital nerve blocks provide rapid relief for occipitally predominant cervicogenic headache and can be performed in office settings with minimal risk. Cervical facet joint injections and medial branch nerve blocks provide both diagnostic confirmation and therapeutic relief for facet-mediated cervicogenic headache. Radiofrequency denervation of the medial branches innervating the responsible facet joints — producing controlled thermal ablation of the pain-transmitting nerves — provides durable relief lasting twelve to twenty-four months in the majority of patients with confirmed facet-mediated cervicogenic headache, and can be repeated when pain returns as the denervated nerves regenerate.
Physical Rehabilitation
Physical therapy is the most important and evidence-supported non-pharmacological intervention for cervicogenic headache and should be initiated concurrently with pharmacological management rather than sequentially after medication trials. The specific components of physical therapy most effective for cervicogenic headache include cervical manual therapy and mobilization techniques directed at the dysfunctional upper cervical segments, deep cervical flexor muscle retraining to restore the motor control deficits that characterize cervicogenic headache patients, and postural correction exercises addressing the forward head posture that increases mechanical loading on the upper cervical structures.
High-quality randomized controlled trials comparing cervical manual therapy, exercise, and their combination for cervicogenic headache consistently demonstrate significant reductions in headache frequency, intensity, and duration, with combination therapy producing better outcomes than either approach alone. The effects of physical therapy for cervicogenic headache, unlike pharmacological treatments, tend to be durable beyond the treatment period — reflecting the genuine structural and functional improvements in cervical mechanics that effective rehabilitation produces. Patients who order fioricet online with rx as a short-term acute management support during the initial phase of their cervicogenic headache treatment should be counseled that the goal of their overall management is to reduce reliance on pharmacological acute treatment as physical rehabilitation addresses the underlying cervical dysfunction driving their headache.
Temporomandibular joint disorder-related headache and facial pain is a condition of extraordinary clinical complexity, arising from the dysfunction of one of the most mechanically demanding […]
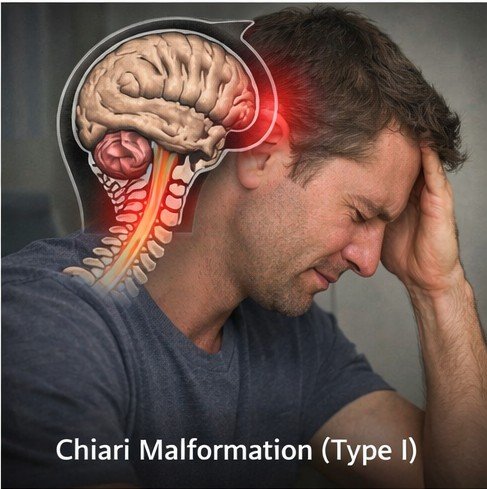
Chiari malformation Type I is a structural neurological condition defined by the downward displacement of the cerebellar tonsils — the lower rounded portions of the […]
Chronic migraine — defined by the International Headache Society as migraine occurring on fifteen or more days per month for at least three months, with […]