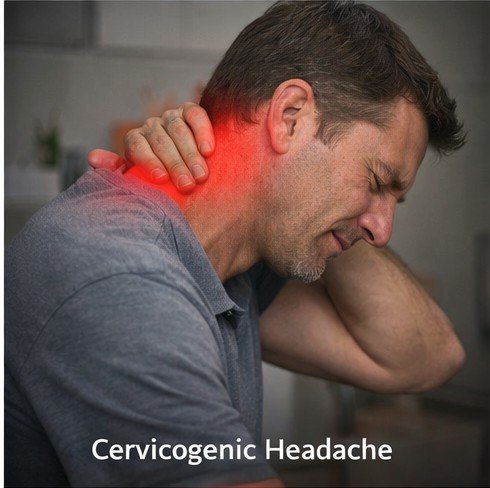
The neck bears the weight of the head — averaging approximately five kilograms — through a complex architecture of vertebrae, intervertebral discs, facet joints, ligaments, and muscles that must simultaneously provide stability, protect the spinal cord, and allow an extraordinary range of motion. When this architecture fails — through trauma, degeneration, inflammatory disease, or the postural stresses of modern sedentary work — the consequences can extend far beyond the neck itself. Cervicogenic headache is a distinct secondary headache disorder in which pain originating from cervical spine structures is referred to the head through shared neural pathways, producing chronic headache that closely mimics primary headache disorders and is routinely misdiagnosed as migraine or tension-type headache.
The condition accounts for an estimated four to twenty percent of chronic headache cases in specialty settings, making it far more prevalent than many clinicians appreciate. Patients with cervicogenic headache may spend years receiving treatments designed for primary headache conditions — triptans, migraine preventives, empirical pharmacological management — without addressing the cervical pathology generating their pain. Accurate diagnosis followed by appropriately targeted cervical treatment dramatically changes the clinical trajectory for these patients, often achieving relief that years of migraine-directed therapy failed to provide.
Anatomy and Pain Referral
Cervicogenic headache is fundamentally a referred pain phenomenon. The anatomical basis lies in the convergence of nociceptive signals from upper cervical structures with signals from cranial structures within the trigeminal nucleus caudalis in the caudal brainstem. The upper three cervical nerve roots — C1, C2, and C3 — innervate the atlantooccipital and atlantoaxial joints, the upper cervical facet joints, and the suboccipital musculature. Pain signals from these structures enter the trigeminal nucleus caudalis and converge with afferent signals from cranial territories including the occiput, vertex, temples, periorbital area, and forehead.
This convergence creates the defining feature of cervicogenic headache: pain that is generated in the neck but perceived in the head. The upper cervical facet joints — particularly the C2-C3 zygapophyseal joint innervated by the third occipital nerve — are among the most commonly implicated pain generators. The suboccipital muscles develop myofascial trigger points under chronic loading that refer pain to the occiput and vertex. The greater occipital nerve, formed primarily from the C2 dorsal ramus, traverses the suboccipital musculature and is frequently entrapped or irritated in this region, generating occipital and hemicranial pain that is sometimes confused with occipital neuralgia.
Causes and Risk Factors
Whiplash injury is among the most common precipitants, with post-traumatic cervicogenic headache developing in a significant proportion of patients following rear-end motor vehicle collisions. The rapid acceleration-deceleration forces applied to the cervical spine in whiplash load the upper cervical facet joints and ligamentous structures beyond their physiological range, producing articular microtrauma and ligamentous injury that may evolve into chronic cervicogenic pain. Cervical spondylosis — age-related degenerative changes in the discs, vertebral endplates, and facet joints — is the most common cause in middle-aged and older patients, with upper cervical facet arthrosis generating referred pain to the head.
Forward head posture — the cervical alignment abnormality associated with prolonged screen use and desk work — is increasingly recognized as a driver of cervicogenic headache in younger populations. Each inch of forward displacement of the head from its neutral position over the shoulders increases the effective load on the cervical facet joints and suboccipital muscles by approximately ten pounds, progressively accelerating degenerative changes and myofascial dysfunction. The epidemic of smartphone and computer use has made forward head posture ubiquitous, and the resulting rise in cervicogenic headache in younger age groups reflects this postural trend.
Diagnosis
The clinical features of cervicogenic headache include: unilateral pain beginning in the occipital or suboccipital region and radiating forward to the ipsilateral temple, forehead, or periorbital area; provocation or worsening by neck movements or sustained head positions; associated ipsilateral neck pain and shoulder discomfort; and restriction of cervical range of motion. Reproduction of the characteristic headache by firm manual pressure on the upper cervical facet joints during physical examination provides strong diagnostic support.
Cervical spine MRI and CT identify structural pathology including disc herniation, facet arthrosis, and ligamentous injury that may correlate with the clinical presentation. Diagnostic nerve blocks — injecting local anesthetic around the third occipital nerve, the C2 dorsal root ganglion, or the upper cervical facet joints — confirm the cervical origin of headache by producing temporary complete relief of the characteristic pain pattern. A positive response to a properly performed diagnostic block, with appropriate volume controls and placebo controls where feasible, is the most reliable confirmation of cervicogenic headache.
Treatment
Physical therapy targeting the specific cervical segment implicated in pain generation is the cornerstone of conservative management. High-velocity low-amplitude manipulation and mobilization of the upper cervical joints has strong evidence for reducing cervicogenic headache frequency and intensity. Deep cervical flexor muscle strengthening — these muscles are consistently inhibited and weak in cervicogenic headache patients — produces durable improvements when practiced consistently. Manual therapy directed at suboccipital trigger points and myofascial restrictions provides additional pain relief and complements joint-directed techniques.
Interventional procedures are highly effective for patients not responding to conservative management. Third occipital nerve blocks and C2-C3 facet joint injections provide both diagnostic confirmation and therapeutic benefit. For patients whose pain is confirmed to arise from a specific facet joint through diagnostic blocking, radiofrequency ablation of the medial branch nerves innervating that joint can provide relief lasting twelve to twenty-four months per treatment cycle. Greater occipital nerve blocks provide rapid, significant relief for the occipital and hemicranial pain components and can serve as both treatment and diagnostic confirmation.
Pharmacological management during flares addresses acute pain while other modalities work on the underlying pathology. For severe episodes unresponsive to NSAIDs or muscle relaxants, a physician may recommend stronger combination analgesics on a strictly limited basis. Patients directed to buy fioricet online with rx for this purpose should understand that in cervicogenic headache — which has a strong tendency toward chronification — the risk of developing medication overuse headache is substantial, and frequency must be rigorously maintained within the prescribed limits, typically no more than two days per week. Purchasing fioricet at the pharmacy with a valid prescription and taking advantage of pharmacist counseling on usage limits is an important safety measure that complements the broader cervicogenic management plan.
Ergonomic modification is essential for patients whose cervicogenic headache is driven or perpetuated by postural loading. Monitor height adjustment to eye level, lumbar and cervical support in seating, regular movement breaks, and reduced smartphone screen time collectively reduce the cumulative cervical mechanical stress that drives symptom recurrence. These modifications are among the most practical and cost-effective interventions available and should be implemented in parallel with therapeutic and interventional approaches rather than deferred until other treatments have been tried.
The prognosis for cervicogenic headache with comprehensive management is favorable. Accurate diagnosis — identifying the specific cervical structures generating pain — and directing treatment precisely at those structures, rather than managing headache empirically, is the key to achieving results that stand in marked contrast to what years of misdirected primary headache treatment typically provide. Most patients achieve substantial improvement in headache frequency and severity with a combination of targeted physical therapy, interventional procedures when indicated, and postural ergonomic modification.
The Paradox at the Heart of Rebound Headache Few medical phenomena are as counterintuitive as medication overuse headache, commonly known as rebound headache. The very […]
Defining Post-Traumatic Headache Post-traumatic headache is the most common symptom following traumatic brain injury and concussion, affecting between 30 and 90 percent of individuals who […]
The temporomandibular joint connects the lower jaw to the temporal bone of the skull and is among the most mechanically complex joints in the human […]