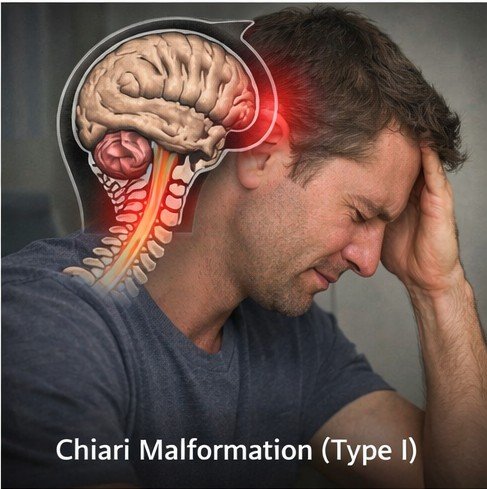
Chiari malformation Type I is a structural neurological condition defined by the downward displacement of the cerebellar tonsils — the lower rounded portions of the cerebellum — through the foramen magnum, the large opening at the base of the skull through which the brainstem continues into the spinal cord. When the cerebellar tonsils extend more than five millimeters below the foramen magnum, they occupy space in the upper cervical spinal canal, potentially obstructing the normal oscillatory flow of cerebrospinal fluid between the cranial cavity and the spinal canal. The result is a spectrum of neurological symptoms of which headache is the most prominent and diagnostically characteristic.
The widespread availability of MRI has revealed that radiographic Chiari I findings are more prevalent than historically appreciated, appearing in approximately one percent of individuals undergoing brain MRI. Not all of these individuals are symptomatic, and the decision to treat is driven by clinical presentation rather than imaging thresholds alone. For symptomatic patients, headache management — both during the period of evaluation and decision-making and as a long-term strategy in those managed conservatively — is a central clinical challenge requiring careful individualization.
The Physiology of Chiari Headache
The headache of Chiari malformation arises from a distinct and well-understood mechanism that differs fundamentally from the mechanisms underlying primary headache disorders. The cerebellar tonsils, by partially occluding the foramen magnum, reduce the free movement of CSF that normally occurs with every cardiac systole and respiratory cycle. Each arterial pulse wave entering the cranial vault generates a compensatory CSF pressure wave that should travel freely between the cranial and spinal compartments through the foramen magnum. When this transit is impeded by descended cerebellar tissue, the resulting pressure is transmitted to pain-sensitive dural and bony structures in the posterior cranial fossa and upper cervical canal.
The Valsalva maneuver — coughing, sneezing, straining, heavy lifting, or any activity that transiently elevates intrathoracic pressure — amplifies these pressure phenomena dramatically by simultaneously increasing venous engorgement of the epidural venous plexus, further narrowing the already compromised CSF pathway. The result is the pathognomonic headache of Chiari malformation: a sudden, explosive, pressure-type pain in the occipital or suboccipital region that is consistently and specifically triggered by Valsalva activities and lasts seconds to a few minutes.
Syringomyelia — a fluid-filled cavity within the spinal cord — develops as a secondary complication in a significant proportion of symptomatic Chiari patients due to the distorted CSF dynamics at the craniocervical junction. Its presence produces additional symptoms including dissociated sensory loss, upper or lower limb weakness, and in severe or long-standing cases autonomic and sphincter dysfunction. Syringomyelia is one of the strongest indications for surgical intervention and represents the most important long-term complication of untreated symptomatic Chiari malformation.
Clinical Presentation and Diagnosis
Beyond the characteristic Valsalva-provoked headache, many patients with symptomatic Chiari I experience a chronic baseline occipital and suboccipital ache, neck pain, and a variety of neurological symptoms reflecting pressure on brainstem and upper cervical cord structures. These may include balance difficulties, oscillopsia, dysphagia, hoarseness, tinnitus, facial numbness, and hearing changes. The overlap between these symptoms and those of multiple sclerosis, posterior fossa tumors, and other neurological conditions makes the MRI finding of tonsillar descent particularly important for establishing the diagnosis.
MRI of the brain and cervical spine is the definitive diagnostic study. Phase-contrast MRI assesses CSF flow dynamics at the craniocervical junction, providing functional information about whether the tonsillar descent is producing hemodynamically significant obstruction — a key variable in surgical decision-making. Patients with clinical symptoms consistent with Chiari malformation should undergo formal ophthalmological assessment and audiological evaluation to characterize the full extent of cranial nerve involvement.
For patients not meeting criteria for surgical intervention — mild symptoms, borderline tonsillar descent, preserved CSF flow on phase-contrast MRI — conservative medical management of headache is an important aspect of care. Practical measures reducing Valsalva-provoked episodes include stool softeners to prevent constipation-related straining, avoidance of heavy lifting and contact sports, and management of chronic cough. Neck-strengthening exercises supporting the craniocervical junction may reduce baseline occipital discomfort.
Pharmacological management requires individualization. Simple analgesics and NSAIDs address mild-to-moderate chronic occipital pain. For more severe acute episodes, physicians managing Chiari patients sometimes recommend short-term use of stronger combination analgesics as bridging support while pressure-reducing measures are being evaluated. Patients who are advised to buy fioricet with medical prescription for breakthrough pain during severe Chiari-related episodes should receive explicit counseling about the strict frequency limits applicable to butalbital-containing medications — typically no more than two days per week — given the chronic pain substrate inherent to this neurological condition and the consequent vulnerability to medication overuse headache. Those managing their prescriptions remotely may order fioricet online with rx through licensed telehealth services, provided clinical evaluation requirements are met.
Acetazolamide — a carbonic anhydrase inhibitor that reduces CSF production — has been used as a temporizing measure in some patients with Chiari malformation, though robust evidence for this specific application is limited. It may serve a role in patients awaiting surgical evaluation or in those with mild pressure-related symptoms where reducing CSF production volume offers theoretical benefit.
Surgical Management and Outcomes
Posterior fossa decompression — removal of a portion of the occipital bone and typically the C1 posterior arch, with or without duraplasty — is the standard surgical treatment for symptomatic Chiari malformation. The Valsalva-provoked headache component responds most reliably to decompression, with the majority of operated patients reporting significant improvement or complete resolution. Chronic baseline occipital pain also improves substantially in most cases. Neurological symptoms attributable to brainstem compression or syringomyelia may stabilize or gradually improve, with syrinx collapse typically occurring progressively over months following successful decompression.
Patient selection is critical. Surgery should be reserved for patients with clearly symptomatic disease and imaging evidence of significant tonsillar descent with or without demonstrable CSF flow obstruction. Incidentally found Chiari I in an asymptomatic individual does not warrant intervention, but does warrant periodic clinical review and patient education about the symptoms that should prompt return for reassessment. Long-term MRI surveillance monitors for changes in tonsillar position, syrinx evolution, and symptom trajectory regardless of management approach.
For patients in the peri-operative period, adequate pain control is important for comfort and rehabilitation participation. Surgeons and neurologists coordinating peri-surgical care may include combination analgesics in the acute pain management plan. Patients directed to purchase fioricet after the doctor visit as part of this plan should receive clear written instructions regarding dosing frequency and duration limits, and should be advised to contact their provider if headache characteristics change or worsen during recovery.
Fioricet 40mg is a combination prescription medication formulated specifically for the management of tension headaches and, in clinical practice, for certain types of migraine headache […]